TOPOGRAPHIC ANATOMY OF THE UPPER ABDOMINAL CAVITY
The abdominal cavity is a space lined from the inside with intra-abdominal fascia.
Borders: above – the diaphragm, below – the border line, in front – the anterolateral wall, behind – the posterior wall of the abdomen.
Departments:
abdominal (peritoneal) cavity - a space limited by the parietal layer of the peritoneum;
retroperitoneal space - the space located between the parietal peritoneum and the intra-abdominal fascia, lining the posterior wall of the abdomen from the inside.
Peritoneum
The peritoneum is a serous membrane that lines the inside of the abdominal wall and covers most of its organs. Departments:
Parietal(parietal) peritoneum– lines the walls belly.
Visceral peritoneum– covers the abdominal organs.
Options for covering organs with peritoneum:
intraperitoneal - from all sides; mesoperitoneal – on three sides (one side is not
covered); extraperitoneal - on one side.
Properties of the peritoneum : humidity, smoothness, shine, elasticity, bactericidal properties, adhesiveness.
Functions of the peritoneum : fixing, protective, excretory, absorption, receptor, conduction, depository (blood).
Course of the peritoneum
From the anterior abdominal wall, the peritoneum passes to the lower concave surface of the diaphragm, then to the upper
the surface of the liver and forms two ligaments: one in the sagittal plane - the falciform ligament, the second in the frontal plane - the coronary ligament of the liver. From the upper surface of the liver, the peritoneum passes to its lower surface and, approaching the gate of the liver, meets the layer of peritoneum, which goes to the liver from the posterior abdominal wall. Both layers go to the lesser curvature of the stomach and the upper part of the duodenum, forming the lesser omentum. Covering the stomach on all sides, the leaves of the peritoneum descend down from its greater curvature and, turning around, return and approach in front of the transverse colon to the body of the pancreas, forming the greater omentum. In the area of the body of the pancreas, one leaf rises upward, forming the posterior wall of the abdominal cavity. The second leaf goes to the transverse colon, covers it on all sides, returns back, forming the mesentery of the intestine. Then the leaf descends, covers the small intestine on all sides, forms its mesentery and the mesentery of the sigmoid colon and descends into the pelvic cavity.
Floors abdominal cavity
The peritoneal cavity is divided into two floors by the transverse colon and its mesentery:
Top floor– located above the transverse colon intestine and its mesenteries. Contents: liver, spleen, stomach, partially duodenum; right and left hepatic, subhepatic, pregastric and omental bursae.
Ground floor– located below the transverse colon intestine and its mesenteries. Contents: loops of jejunum and ileum; cecum and vermiform appendix;
colon; lateral canals and mesenteric sinuses. The root of the mesentery of the transverse colon goes from right to left from the right kidney, slightly below its middle, to the middle of the left. On its way it crosses: the middle of the descending part of the duodenum; head of the pancreas
of the gland and runs along the upper edge of the gland body.
Upper abdominal bursae
Right hepatic bursa located between the diaphragm and the right lobe of the liver and limited behind the right coronary
ligament of the liver, on the left – the falciform ligament, and on the right and below it opens into the subhepatic bursa and the right lateral canal.
Left hepatic bursa lies between the diaphragm and the left lobe of the liver and is bounded posteriorly by the left coronary ligament of the liver, on the right by the falciform ligament, on the left by the left triangular ligament of the liver, and in front communicates with the pregastric bursa.
Pregastric bursa located between the stomach and the left lobe of the liver and is limited in front by the lower surface of the left lobe of the liver, behind by the lesser omentum and the anterior wall of the stomach, above by the porta hepatis and communicates with the subhepatic bursa and the lower floor of the abdominal cavity through the preepiploic fissure.
Subhepatic bursa it is limited in front and above by the lower surface of the right lobe of the liver, below - by the transverse colon and its mesentery, on the left - by the porta hepatis and on the right it opens into the right lateral canal.
Omental bag forms a closed pocket behind stomach and consists of the vestibule and the gastro-pancreatic sac.
Vestibule of the omental bursa limited at the top of the tail-
that lobe of the liver, in front - the lesser omentum, below - the duodenum, behind - the parietal part of the peritoneum lying on the aorta and the inferior vena cava.
Stuffing box hole bounded in front by the hepatoduodenal ligament, which contains the hepatic artery, common bile duct and portal vein, below by the duodenal-renal ligament, behind by the hepatorenal ligament, above by the caudate lobe of the liver.
Gastrointestinal- pancreas pouch limited front rear
the lower surface of the lesser omentum, the posterior surface of the stomach and the posterior surface of the gastrocolic ligament, behind - the parietal peritoneum lining the pancreas, aorta and inferior vena cava, above - the caudate lobe of the liver, below - the mesentery of the transverse colon, on the left - the gland - splenic and renal-splenic ligaments.
Topographic anatomy of the stomach Holotopia: left hypochondrium, epigastric region proper -
Skeletotopia:
cardiac foramen – to the left of Th XI (behind the cartilage of the VII rib);
bottom – Th X (V rib along the left midclavicular line); pylorus – L1 (VIII right rib in the midline).
Syntopy: at the top – the diaphragm and the left lobe of the liver, at the back
on the left - the pancreas, left kidney, adrenal gland and spleen, in front - the abdominal wall, below - the transverse colon and its mesentery.
Gastric ligaments:
Hepatic- gastric ligament– between the porta hepatis and lesser curvature of the stomach; contains the left and right gastric arteries, veins, branches of the vagus trunks, lymphatic vessels and nodes.
Diaphragmatically- esophageal ligament– between the diaphragm
esophagus and cardiac part of the stomach; contains a branch of the left gastric artery.
Gastrointestinal- diaphragmatic ligament is formed as a result transition of the parietal peritoneum from the diaphragm to the anterior wall of the fundus and partially the cardiac part of the stomach.
Gastrointestinal- splenic ligament– between the spleen and greater curvature of the stomach; contains short arteries and veins of the stomach.
Gastrointestinal- colic ligament– between greater curvature stomach and transverse colon; contains the right and left gastroepiploic arteries.
Gastrointestinal- pancreatic ligament is formed during the transition
de peritoneum from the upper edge of the pancreas to the posterior wall of the body, cardia and fundus of the stomach; contains the left gastric artery.
Blood supply to the stomach provided by the celiac axis system.
Left gastric artery is divided into ascending esophageal and descending branches, which, passing along the lesser curvature of the stomach from left to right, give off anterior and posterior branches.
Right gastric artery starts from own hepatic artery. As part of the hepatoduodenal ligament, the artery reaches the pyloric
The lower part of the stomach and between the leaves of the lesser omentum along the lesser curvature is directed to the left towards the left gastric artery, forming the arterial arch of the lesser curvature of the stomach.
Left gastro- omental artery is a branch splenic artery and is located between the leaves of the gastrosplenic and gastrocolic ligaments along the greater curvature of the stomach.
Right gastrointestinal- omental artery starts from gastroduodenal artery and goes from right to left along the greater curvature of the stomach towards the left gastroepiploic artery, forming a second arterial arch along the greater curvature of the stomach.
Short gastric arteries in quantity 2-7 branches depart from the splenic artery and, passing in the gastrosplenic ligament, reach the bottom along the greater curvature
The veins of the stomach accompany the arteries of the same name and flow into the portal vein or one of its roots.
Lymphatic drainage
The efferent lymphatic vessels of the stomach empty into the first-order lymph nodes located in the lesser omentum, located along the greater curvature, at the hilum of the spleen, along the tail and body of the pancreas, into the subpyloric and superior mesenteric lymph nodes. The drainage vessels from all of the listed first-order lymph nodes are directed to the second-order lymph nodes, which are located near the celiac trunk. From them, lymph flows into the lumbar lymph nodes.
Innervation of the stomach provided by the sympathetic and parasympathetic parts of the autonomic nervous system. The main sympathetic nerve fibers are directed to the stomach from the celiac plexus, enter and spread in the organ along extra- and intraorgan vessels. Parasympathetic nerve fibers into the stomach come from the right and left vagus nerves, which form the anterior and posterior vagus trunks below the diaphragm.
Topographic anatomy of the duodenum Holotopia: in the epigastric and umbilical regions.
The duodenum has four sections: superior, descending, horizontal and ascending.
Top part ( bulb ) duodenum located between the pylorus of the stomach and the superior flexure of the duodenum.
Relation to the peritoneum: covered intraperitoneally in the initial part, mesoperitoneally in the middle part.
Skeletotopia– L1.
Syntopy: above the gallbladder, below is the head of the pancreas, in front is the antrum of the stomach.
Descending part the duodenum forms more or less pronounced bend to the right and goes from the upper to the lower bends. The common bile duct and the pancreatic duct on the major duodenal papilla open into this part. A little higher than it there may be a non-permanent small duodenal papilla, on which the accessory duct of the pancreas opens.
Relation to the peritoneum:
Skeletotopia– L1-L3.
Syntopy: on the left is the head of the pancreas, behind and on the right is the right kidney, right renal vein, inferior vena cava and ureter, in front is the mesentery of the transverse colon and loops of the small intestine.
Horizontal part duodenum goes from the inferior bend to the intersection with the superior mesenteric vessels.
Relation to the peritoneum: located retroperitoneally.
Skeletotopia– L3.
Syntopy: superiorly the head of the pancreas, behind inferior vena cava and abdominal aorta, anterior and inferior loops of the small intestine.
Rising part The duodenum extends from the intersection with the superior mesenteric vessels to the left and up to the duodenojejunal flexure and is fixed by the suspensory ligament of the duodenum.
Relation to the peritoneum: located mesoperitoneally.
Skeletotopia– L3-L2.
Syntopy: above the lower surface of the body of the pancreas, behind the inferior vena cava and abdominal aorta, in front and below the loops of the small intestine.
Duodenal ligaments
Hepatic- duodenal ligament– between the gates liver and the initial part of the duodenum and contains its own hepatic artery, located in the ligament on the left, the common bile duct located on the right, and between them and behind – the portal vein.
Duodenum- renal ligament in the form of a fold of the belly
The splint is stretched between the outer edge of the descending part of the intestine and the right kidney.
Blood supply to the duodenum provide
It comes from the system of the celiac trunk and the superior mesenteric artery.
Posterior and anterior superior pancreas- twelve-
duodenal arteries arise from the gastroduodenal arteries.
Rear and anterior inferior pancreas-
duodenal arteries arise from the superior mesenteric arteries, go towards the two upper ones and connect with them.
The veins of the duodenum follow the course of the arteries of the same name and drain blood into the portal vein system.
Lymphatic drainage
The draining lymphatic vessels empty into the first-order lymph nodes, which are the superior and inferior pancreaticoduodenal nodes.
Innervation duodenum is carried out from the celiac, superior mesenteric, hepatic and pancreatic nerve plexuses, as well as branches of both vagus nerves.
Intestinal suture
Intestinal suture is a collective concept that unites all types of sutures that are placed on hollow organs (food, stomach, small and large intestines).
Primary requirements, presented to the intestinal suture:
Tightness– is achieved by contact of the serous membranes of the stitched surfaces.
Hemostatic– is achieved by capturing the submucosal base of a hollow organ into the suture (the suture should provide hemostasis, but without significant disruption of the blood supply to the organ wall along the suture line).
Adaptability– the seam must be made taking into account case structure of the walls of the digestive tract for optimal comparison with each other of the same membranes of the intestinal tube.
Strength– is achieved by capturing the submucosal layer into the suture, where a large number of elastic fibers are located.
Asepsis(purity, non-infection) – this requirement is met if the mucous membrane of the organ is not captured in the suture (using “clean” single-row sutures or immersing through (infected) sutures with a “clean” seromuscular suture).
The wall of the hollow organs of the abdominal cavity has four main layers: mucous membrane; submucosal layer; muscle layer; serous layer.
The serous membrane has pronounced plastic properties (the surfaces of the serous membrane brought into contact with the help of sutures are firmly glued together after 12-14 hours, and after 24-48 hours the connected surfaces of the serous layer firmly grow together). Thus, the application of sutures that bring the serous membrane closer together ensures the tightness of the intestinal suture. The frequency of such seams should be at least 4 stitches per 1 cm of the length of the stitched area. The muscular layer gives elasticity to the suture line and therefore its grasping is an indispensable attribute of almost any type of intestinal suture. The submucosal layer provides the mechanical strength of the intestinal suture, as well as good vascularization of the suture area. Therefore, the connection of the edges of the intestine is always carried out with the capture of the submucosa. The mucous membrane does not have mechanical strength. The connection of the edges of the mucous membrane ensures good adaptation of the wound edges and protects the suture line from the penetration of infection from the lumen of the organ.
Classification of intestinal sutures
Depending on the application method
manual;
mechanical– applied with special devices;
combined.
Depending on , what layers of the gripping wall - fit into the seam
gray- serous; serous- muscular;
slimy- submucosal; seriously- muscularly- submucosal;
serous- muscularly- submucosal- mucous membranes(end-to-end).
Through seams are infected (“dirty”).
Sutures that do not pass through the mucous membrane are called non-infected (“clean”).
Depending on the row of intestinal sutures
single row seams(Bira-Pirogova, Mateshuka) – a thread passes through the edges of the serous, muscular membranes and submucosa (without capturing the mucous membrane), which ensures good adaptation of the edges and reliable immersion into the lumen of the intestinal mucosa without additional trauma to it;
double row seams(Alberta) – used as the first row is a through suture, on top of which (in the second row) a seromuscular suture is applied;
three-row seams– used as first a row of a through suture, over which seromuscular sutures are applied in the second and third rows (usually used for application to the large intestine).
Depending on the characteristics of the sutures through the wall of the wound edge
edge seams; screw-in seams;
everting sutures; combined screwing- eversible seams.
By application method
nodal; continuous.
STOMACH OPERATIONS
Surgical interventions performed on the stomach are divided into palliative and radical. Palliative operations include: suturing a perforated gastric ulcer, gastrostomy and gastroenteroanastomosis. Radical operations on the stomach include removal of part (resection) or the entire stomach (gastrectomy).
Palliative operations on the stomach Gastrostomy– application of artificial gastric fistula
Indications : injuries, fistulas, burns and scar contractions esophagus, inoperable cancer of the pharynx, esophagus, cardia of the stomach.
Classification :
tubular fistulas– to create and operate a rubber tube is used (Witzel and Strain-Senna-Kader methods); are temporary and, as a rule, close on their own after the tube is removed;
labiform fistulas– artificial entrance is formed from stomach walls (Topver method); are permanent, since they require surgery to close them.
Gastrostomy according to Witzel
transrectal left-sided layer-by-layer laparotomy 10-12 cm long from the costal arch down;
removal of the anterior wall of the stomach into the wound, onto which a rubber tube is placed between the lesser and greater curvatures along the long axis, so that its end is located in the area of the pyloric region;
application of 6-8 interrupted seromuscular sutures on both sides of the tube;
immersing the tube into the gray-serous canal formed by the anterior wall of the stomach by tying sutures;
placing a purse-string suture in the area of the pylorus, opening the stomach wall inside the suture, inserting the end of the tube into the stomach cavity;
tightening the purse-string suture and placing 2-3 seromuscular sutures over it;
removing the other end of the tube through a separate incision along the outer edge of the left rectus muscle;
fixation of the stomach wall (gastropexy) along the formed edge to the parietal peritoneum and to the posterior wall of the rectus sheath with several seromuscular sutures.
Gastrostomy according to Stamm- Senna- Kadera
transrectal access; removal of the anterior wall of the stomach into the wound and application
closer to the cardia of three purse-string sutures (in children there are two) at a distance of 1.5-2 cm from each other;
opening the stomach cavity in the center of the internal purse-string suture and inserting a rubber tube;
sequential tightening of purse-string sutures, starting from the inner;
removal of the tube through an additional soft tissue incision;
gastropexy.
When creating tubular fistulas, it is necessary to carefully fix the anterior wall of the stomach to the parietal peritoneum. This stage of the operation allows you to isolate the abdominal cavity from the external environment and prevent serious complications.
Lip gastrostomy according to Topver
quick access; removal of the anterior wall of the stomach into the surgical wound
in the form of a cone and placing 3 purse string sutures on it at a distance of 1-2 cm from each other, without tightening them;
dissection of the stomach wall at the top of the cone and insertion of a thick tube inside;
alternately tightening the purse-string sutures, starting from the outer one (a corrugated cylinder is formed around the tube from the wall of the stomach, lined with the mucous membrane);
suturing the stomach wall at the level of the lower purse-string suture to the parietal peritoneum, at the level of the second suture - to
the sheath of the rectus abdominis muscle, at the third level - to the skin;
Upon completion of the operation, the tube is removed and inserted only during feeding.
Gastroenterostomy(the junction between the stomach and the small intestine) is performed when the patency of the pyloric part of the stomach is impaired (inoperable tumors, cicatricial stenosis, etc.) in order to create an additional path for the drainage of gastric contents into the jejunum. Depending on the position of the intestinal loop in relation to the stomach and transverse colon, the following types of gastroenteroanastomosis are distinguished:
anterior anterior colonic gastroenteroanastomosis;
posterior anterior colonic gastroenteroanastomosis;
anterior retrocolic gastroenteroanastomosis;
posterior retrocolic gastrojejunostomy. The first and fourth variants of the operation are most often used.
When applying the anterior anterior rim anastomosis, 30-45 cm are removed from the flexura duodenojejunalis (long-term anastomosis)
loop) and additionally, in order to prevent the development of a “vicious circle,” an anastomosis is formed between the afferent and efferent loops of the jejunum according to the “side to side” type. When a posterior retrocolic anastomosis is applied, 7-10 cm are removed from the flexura duodenojejunalis (short loop anastomosis). For the correct functioning of anastomoses, they are applied isoperistaltically (the afferent loop should be located closer to the cardiac part of the stomach, and the efferent loop should be closer to the antrum).
Severe complication after surgery to apply a gastrointestinal anastomosis - “ vicious circle"- occurs, most often, with anterior anastomosis with a relatively long loop. The contents from the stomach enter in the antiperistaltic direction into the adductor knee of the jejunum (due to the predominance of the motor force of the stomach) and then back to the stomach. Reasons This formidable complication is: incorrect suturing of the intestinal loop in relation to the axis of the stomach (in the antiperistaltic direction) and the formation of the so-called “spur”.
To avoid the development of a vicious circle due to the formation of a “spur,” the adducting end of the jejunum is strengthened to the stomach with additional seromuscular sutures 1.5-2 cm above the anastomosis. This prevents the intestine from bending and forming a “spur”.
Suturing of a perforated ulcer of the stomach and duodenum
With a perforated gastric ulcer, two types of urgent surgical interventions are possible: suturing the perforated ulcer or resection of the stomach along with the ulcer.
Indications for suturing a perforated ulcer :
sick children and young people; in persons with a short history of ulcers;
in elderly people with concomitant pathologies (cardiovascular failure, diabetes mellitus, etc.);
if more than 6 hours have passed since the perforation; with insufficient experience of the surgeon.
When suturing a perforation hole, it is necessary
adhere to the following rules:
a defect in the wall of the stomach or duodenum is usually sutured with two rows of Lambert seromuscular sutures;
the suture line should be directed perpendicular to the longitudinal axis of the organ (to avoid stenosis of the lumen of the stomach or duodenum);
Radical gastric surgery
Radical operations include gastric resection and gastrectomy. The main indications for performing these interventions are: complications of gastric and duodenal ulcers, benign and malignant tumors of the stomach.
Classification :
Depending on the location of the part of the organ being removed:
proximal resections(the cardiac part and part of the body of the stomach are removed);
distal resections(the antrum is removed and part of the body of the stomach).
Depending on the volume of the stomach part removed:
economical - resection of 1/3-1/2 of the stomach;
extensive – resection of 2/3 of the stomach;
subtotal – resection of 4/5 of the stomach.
Depending on the shape of the part of the stomach being removed:
wedge-shaped;
stepped;
circular.
Stages of gastric resection
Mobilization(skeletonization) the part being removed-
Ludka– intersection of the gastric vessels along the small and large curvature between the ligatures throughout the resection area. Depending on the nature of the pathology (ulcer or cancer), the volume of the removed part of the stomach is determined.
Resection– the part planned for resection is removed stomach.
Restoring the continuity of the digestive tube( gastroduodenoanastomosis or gastroenteroanastomosis ).
In this regard, there are two main types of opera-
The operation according to the Billroth-1 method is the creation of an “end to end” anastomosis between the stump of the stomach and the stump of the duodenum.
Operation according to the Billroth-2 method - formation of a side-to-side anastomosis between the gastric stump and the jejunal loop, closure of the duodenal stump ( in class-
not applicable).
The operation using the Billroth-1 method has an important advantage compared to the Billroth-2 method: it is physiological, because The natural passage of food from the stomach to the duodenum is not disrupted, i.e. the latter is not excluded from digestion.
However, the Billroth-1 operation can be completed only with “small” gastric resections: 1/3 or antrum resection. In all other cases, due to anatomical features (due to
peritoneal location of most of the duodenum and fixation of the gastric stump to the esophagus), it is very difficult to form a gastroduodenal anastomosis (there is a high probability of sutures coming apart due to tension).
Currently, for resection of at least 2/3 of the stomach, the Billroth-2 operation, modified by Hoffmeister-Finsterer, is used. The essence of this modification is as follows:
the stump of the stomach is connected to the jejunum using an end-to-side anastomosis;
the width of the anastomosis is 1/3 of the lumen of the gastric stump;
the anastomosis is fixed in the “window” of the mesentery of the transverse colon;
The afferent loop of the jejunum is sutured with two or three interrupted sutures to the stump of the stomach to prevent the reflux of food masses into it.
The most important disadvantage of all modifications of the Billroth-2 operation is the exclusion of the duodenum from digestion.
5-20% of patients who have undergone gastrectomy develop diseases of the “operated stomach”: dumping syndrome, afferent loop syndrome (reflux of food masses into the afferent loop of the small intestine), peptic ulcers, cancer of the gastric stump, etc. Often such patients have to be operated on again - to perform reconstructive surgery, which has two goals: removal of the pathological focus (ulcer, tumor) and inclusion of the duodenum in digestion.
For advanced gastric cancer, perform gastrek- Tomia– removal of the entire stomach. It is usually removed together with the greater and lesser omentum, spleen, tail of the pancreas and regional lymph nodes. After removal of the entire stomach, the continuity of the digestive canal is restored by gastric plastic surgery. Plastic surgery of this organ is performed using a loop of the jejunum, a segment of the transverse colon, or other parts of the colon. The small or large intestinal insert is connected to the esophagus and duodenum, thus restoring the natural passage of food.
Vagotomy– dissection of the vagus nerves.
Indications : complicated forms of duodenal ulcer and pyloric stomach, accompanied by penetration and perforation.
Classification
Truncal vagotomy– intersection of the trunks of the vagus nerves before the origin of the hepatic and splanchnic nerves. Leads to parasympathetic denervation of the liver, gallbladder, duodenum, small intestine and pancreas, as well as gastrostasis (performed in combination with pyloroplasty or other drainage operations)
supradiaphragmatic; subphrenic.
Selective vagotomy– lies in the intersection trunks of the vagus nerves going to the entire stomach, after separating the branches of the hepatic and celiac nerves.
Selective proximal vagotomy– cross-
There are branches of the vagus nerves that go only to the body and fundus of the stomach. The branches of the vagus nerves innervating the antrum of the stomach and pylorus (Laterger branch) do not cross. The Laterger branch is considered purely motor, which regulates the motor activity of the forearm.
ric sphincter of the stomach.
Drainage operations on the stomach
Indications: ulcerative pyloric stenosis, duodenal bulbs and subbulbous section.
Pyloroplasty – surgery to expand the pyloric opening of the stomach while maintaining or restoring the pyloric closing function.
Heinecke's method – Mikulich – is to
longitudinal dissection of the pyloric part of the stomach and the initial part of the duodenum, 4 cm long, followed by cross-stitching of the resulting wound.
Finney's method – dissect the antrum stomach and the initial part of the duodenum with a continuous arcuate incision and
sutures are placed on the wound according to the principle of upper gastroduodenoanastomosis “side to side”.
Gastroduodenostomy
Jaboley's method – applies if available obstacles in the pyloroantral zone; A side-to-side gastroduodenoanastomosis is performed, bypassing the site of the obstruction.
Gastrojejunostomy – application of classic gastroenteroanastomosis to “off”.
Features of the stomach in newborns and children
In newborns, the stomach is round in shape, its pyloric, cardiac sections and fundus are poorly expressed. The growth and formation of the stomach sections is uneven. The pyloric part begins to stand out only by 2-3 months of a child’s life and develops by 4-6 months. The area of the fundus of the stomach is clearly defined only by 10-11 months. The muscular ring of the cardiac section is almost absent, which is associated with a weak closure of the entrance to the stomach and the possibility of backflow of stomach contents into the esophagus (regurgitation). The cardiac part of the stomach is finally formed by the age of 7-8 years.
The mucous membrane of the stomach in newborns is thin, the folds are not pronounced. The submucosal layer is rich in blood vessels and has little connective tissue. The muscle layer is poorly developed in the first months of life. The arteries and veins of the stomach in young children differ in that the size of their main trunks and branches of the first and second orders is almost the same.
Developmental defects
Congenital hypertrophic pyloric stenosis– expressed-
severe hypertrophy of the muscular layer of the pylorus with narrowing or complete closure of the lumen by folds of the mucous membrane. The serous membrane and part of the circular muscle fibers of the pylorus along its entire length are dissected in the longitudinal direction, the mucous membrane of the pylorus is bluntly released from the deep muscle fibers until it bulges completely through the incision, the wound is sutured in layers.
Constrictions(strictures) body of the stomach– authority accepts hourglass shape.
Complete absence of stomach. Duplication of the stomach.
Features of the duodenum in newborns- money and children
The duodenum in newborns is often ring-shaped and less often U-shaped. In children of the first years of life, the upper and lower bends of the duodenum are almost completely absent.
The upper horizontal part of the intestine in newborns is higher than the usual level, and only by the age of 7-9 years does it descend to the body of the first lumbar vertebra. The ligaments between the duodenum and neighboring organs in young children are very delicate, and the almost complete absence of fatty tissue in the retroperitoneal space creates the possibility of significant mobility of this section of the intestine and the formation of additional kinks.
Malformations of the duodenum
Atresia– complete absence of lumen (characterized by strong expansion and thinning of the walls of those parts of the intestine that are located above the atresia).
Stenosis– due to localized hypertrophy of the wall, the presence of a valve, membrane in the intestinal lumen, compression of the intestine by embryonic cords, annular pancreas, superior mesenteric artery, and a highly located cecum.
In case of atresia and stenosis of the jejunum and ileum, resection of the atretic or narrowed section of the intestine is performed along with a stretched, functionally defective area for 20-25 cm. In the presence of an irremovable obstacle above the confluence of the common bile and pancreatic ducts, a posterior gastroenteroanastomosis is performed. In case of obstruction in the distal intestine, duodenojejunostomy is used.
Diverticula.
Incorrect position of the duodenum–
mobile duodenum.
Lecture No. 7
Peritoneum, a thin serous membrane with a smooth, shiny, uniform surface, covers the walls of the abdominal cavity, cavitas abdominis, and partially the pelvis, organs located in this cavity. The surface area of the peritoneum is about 20,400 cm 2 and is almost equal to the area of the skin. The peritoneum is formed by the lamina propria, lamina propria, serous membrane and the single-layer squamous epithelium covering it - mesothelium, mesothelium.

lining the walls of the abdomen is called the parietal peritoneum, peritoneum parietale; the peritoneum covering the organs is the visceral peritoneum, peritoneum viscerale. Moving from the walls of the abdominal cavity to the organs and from one organ to another, the peritoneum forms ligaments, ligamenta, folds, plicae, mesenteries, mesenterii.
Due to the fact that the visceral peritoneum covering one or another organ passes into the parietal peritoneum, most organs are fixed to the walls of the abdominal cavity. The visceral peritoneum covers the organs in different ways: on all sides (intraperitoneal), on three sides (mesoperitoneal) or on one side (retro- or extraperitoneal). Organs covered with peritoneum on three sides, located mesoperitoneally, include the partially ascending and descending sections, and the middle part.
Organs located extraperitoneally include (except for its initial section), the pancreas, adrenal glands, .
Organs located intraperitoneally have a mesentery connecting them with the parietal.

Mesentery is a plate consisting of two connected layers of the peritoneum of the duplication. One - free - edge of the mesentery covers the organ (intestine), as if suspending it, and the other edge goes to the abdominal wall, where its leaves diverge in different directions in the form of the parietal peritoneum. Usually between the layers of the mesentery (or ligament) blood vessels, lymphatic vessels and nerves approach the organ. The place where the mesentery begins on the abdominal wall is called the root of the mesentery, radix mesenterii; approaching an organ (for example, the intestine), its leaves diverge on both sides, leaving a narrow strip at the point of attachment - the extraperitoneal field, area nuda.
The serous cover, or serous membrane, tunica serosa, is not directly adjacent to the organ or abdominal wall, but is separated from them by a layer of connective tissue subserosa, tela subserosa, which, depending on its location, has varying degrees of development. Thus, the subserosal base under the serous membrane of the liver, diaphragm, and upper part of the anterior wall of the abdomen is poorly developed and, conversely, significantly developed under the parietal peritoneum lining the posterior wall of the abdominal cavity; for example, in the region of the kidneys, etc., where the peritoneum is very movably connected to the underlying organs or to their parts.
The peritoneal cavity, or peritoneal cavity, cavitas peritonealis, is closed in men, and in women through the fallopian tubes, uterus and communicates with the external environment. The peritoneal cavity is a slit-like space of complex shape, filled with a small amount of serous fluid, liquor peritonei, moisturizing the surface of the organs.
The parietal peritoneum of the posterior wall of the abdominal cavity delimits the peritoneal cavity from the retroperitoneal space, spatium retroperitoneale, in which the retroperitoneal organs, organa retroperitonealia, lie. In the retroperitoneal space, behind the parietal peritoneum, there is the retroperitoneal fascia, fascia retroperitonealis.
The extraperitoneal space, spatium extraperitoneale, is also the retropubic space, spatium retropubicum.
Peritoneal cover and peritonealfolds. The anterior parietal peritoneum, peritoneum parietale anterius, forms a series of folds on the anterior wall of the abdomen. Along the midline there is a median umbilical fold, plica umbilicalis mediana, which stretches from the umbilical ring to the apex; This fold contains a connective tissue cord, which is an obliterated urinary duct, urachus. From the umbilical ring to the lateral walls of the bladder there are medial umbilical folds, plicae umbilicales mediales, in which cords of the empty anterior sections of the umbilical arteries are embedded. Outside these folds are the lateral umbilical folds, plicae umbilicales laterales. They stretch from the middle of the inguinal ligament obliquely upward and inward, towards the back. These folds contain the inferior epigastric arteries, aa. epigastricae inferiores, which nourish the rectus abdominis muscles.


At the base of these folds, pits are formed. On both sides of the median umbilical fold, between it and the medial umbilical fold, above the upper edge of the bladder, there are supravesical fossae, fossae supravesicales. Between the medial and lateral umbilical folds are the medial inguinal fossae, fossae inguinales mediates; outward from the lateral umbilical folds lie the lateral inguinal fossae, fossae inguinales laterales; these pits are located against the deep inguinal rings.
A triangular section of the peritoneum, located above the medial inguinal fossa and bounded on the medial side by the edge of the rectus abdominis muscle, with the lateral - lateral umbilical fold and below - the inner part of the inguinal ligament, is called the inguinal triangle, trigonum inguinale.
The parietal peritoneum, covering the anterior abdomen above the umbilical ring and the diaphragm, passing to the diaphragmatic surface of the liver, forms the falciform (suspensory) ligament of the liver, lig. falciforme hepatis, consisting of two layers of peritoneum (duplicate), located in the sagittal plane. In the free lower edge of the falciform ligament there passes a cord of the round ligament of the liver, lig, teres hepatis. The leaves of the falciform ligament pass posteriorly into the anterior layer of the coronary ligament of the liver, lig. coronarium hepatis. It represents the transition of the visceral peritoneum of the diaphragmatic surface of the liver into the parietal peritoneum of the diaphragm. The posterior leaf of this ligament passes to the diaphragm from the visceral surface of the liver. Both leaves of the coronary ligament converge at their lateral ends and form the right and left triangular ligaments, lig. triangulare dextrum et lig. triangulare sinistrum.
The visceral peritoneum, peritoneum visceralis, of the liver covers the gallbladder on the lower side.
From the visceral peritoneum of the liver, the peritoneal ligament is directed to the lesser curvature of the stomach and the upper part of the duodenum. It is a duplication of the peritoneal layer, starting from the edges of the gate (transverse groove) and from the edges of the fissure of the venous ligament, and is located in the frontal plane. The left part of this ligament (from the fissure of the venous ligament) goes to the lesser curvature of the stomach - this is the hepatogastric ligament, lig, hepatogastricum. It looks like a thin web-like plate. Between the leaves of the hepatogastric ligament, along the lesser curvature of the stomach, pass the arteries and veins of the stomach, a. et v. gastricae, nerves; regional lymph nodes are located here. The right part of the ligament, more dense, goes from the porta hepatis to the upper edge of the pylorus and duodenum; this section is called the hepatoduodenal ligament, lig. hepatoduodenale, and includes the common bile duct, the common hepatic artery and its branches, the portal vein, lymphatic vessels, nodes and nerves. On the right, the hepatoduodenal ligament forms the anterior edge of the omental foramen, foramen epiploicum (omentale). Approaching the edge of the stomach and duodenum, the leaves of the ligament diverge and cover the anterior and posterior walls of these organs.
Both ligaments: hepatogastric and hepatoduodenal - make up the lesser omentum, omentum minus. The non-permanent continuation of the lesser omentum is the hepatocolic ligament, lig. hepatocolicum, connecting the gallbladder with the right flexure of the colon. The falciform ligament and lesser omentum represent ontogenetically the anterior, ventral, mesentery of the stomach.
The parietal peritoneum extends from the left part of the dome of the diaphragm, passing onto the cardiac notch and the right half of the gastric vault, forming a small gastrophrenic ligament, lig. gastrophrenicum.
Between the lower edge of the right lobe of the liver and the adjacent upper end of the right kidney, the peritoneum forms a transitional fold - the hepatorenal ligament, lig. hepatorenal.
The leaves of the visceral peritoneum of the anterior and posterior surfaces of the stomach along its greater curvature continue downward in the form of a greater omentum. The greater omentum, omentum majus, in the form of a wide plate (“apron”) follows down to the level of the upper aperture of the small pelvis. Here the two leaves that form it turn up and return, heading upward behind the descending two leaves. These return leaves are fused with the front leaves. At the level of the transverse colon, all four leaves of the greater omentum adhere to the omental band located on the anterior surface of the intestine. Then the posterior (recurrent) layers of the omentum extend from the anterior ones, connect to the mesentery of the transverse colon, mesocolon transversum, and go together dorsally to the line of attachment of the mesentery along the posterior abdominal wall in the region of the anterior edge of the body of the pancreas.
Thus, a pocket is formed between the anterior and posterior layers of the omentum at the level of the transverse colon. Approaching the anterior edge of the body of the pancreas, the two posterior layers of the omentum diverge: the upper layer passes into the posterior wall of the omental bursa (on the surface of the pancreas) in the form of a parietal layer of the peritoneum, the lower layer passes into the upper layer of the mesentery of the transverse colon.
The section of the greater omentum between the greater curvature of the stomach and the transverse colon is called the gastrocolic ligament, lig. gastrocolicum; this ligament fixes the transverse colon to the greater curvature of the stomach. Between the layers of the gastrocolic ligament along the greater curvature, the right and left gastroepiploic arteries and veins pass, and regional lymph nodes lie.
The greater omentum covers the front of the large and small intestine. A narrow gap is formed between the omentum and the anterior abdominal wall - the preomental space. The greater omentum is the distended dorsal mesentery of the stomach. Its continuation to the left is the gastrosplenic ligament, lig. gastrolienale, and diaphragmatic-splenic ligament, lig. phrenicolienale, which transform into one another.
Of the two layers of the peritoneum of the gastrosplenic ligament, the anterior one passes to the spleen, surrounds it on all sides, and returns back to the gate of the organ in the form of a leaf of the diaphragmatic-splenic ligament. The posterior leaf of the gastrosplenic ligament, having reached the hilum of the spleen, turns directly to the posterior abdominal wall in the form of a second leaf of the diaphragmatic-splenic ligament. As a result, the spleen is, as it were, included laterally in the ligament connecting the greater curvature of the stomach with the diaphragm.
The mesentery of the colon, mesocolon, varies in size in different parts of the colon and is sometimes absent. Thus, the cecum, which has the shape of a bag, is covered with peritoneum on all sides, but it does not have a mesentery. In this case, the vermiform appendix extending from the cecum, also surrounded on all sides by the peritoneum (intraperitoneal position), has a mesentery of the vermiform appendix, mesoappendix, reaching significant sizes. At the junction of the cecum with the ascending colon there is sometimes a small mesentery of the ascending colon, mesocolon ascendens.
Thus, the serous membrane covers the ascending colon on three sides, leaving the posterior wall free (mesoperitoneal position).
The mesentery of the transverse colon begins on the posterior abdominal wall at the level of the descending part of the duodenum, the head and body of the pancreas, and the left kidney; approaching the intestine at the mesenteric ribbon, two layers of the mesentery diverge and surround the intestine in a circle (intraperitoneal). Throughout the entire length of the mesentery from the root to the place of attachment to the intestine, its greatest width is 10-15 cm and decreases towards the bends, where it passes into the parietal layer.


The descending colon, like the ascending colon, is covered with a serous membrane on three sides (mesoperitoneal), and only in the area of the transition to the sigmoid colon is sometimes formed a short mesentery of the descending colon, mesocolon descendens. Only a small portion of the posterior wall of the middle third of the descending colon is not covered by peritoneum.
The mesentery of the sigmoid colon, mesocolon sigmoideum, has a width of 12-14 cm, which varies significantly throughout the colon. The root of the mesentery crosses the bottom of the iliac fossa obliquely to the left and from top to bottom and to the right, the iliacus and psoas muscles, as well as the left common iliac vessels and the left ureter located along the border line; Having rounded the border line, the mesentery crosses the area of the left sacroiliac joint and passes to the anterior surface of the upper sacral vertebrae. At the level of the third sacral vertebra, the mesentery of the sigmoid colon ends at the beginning of the very short mesentery of the rectum. The length of the mesenteric root varies greatly; the steepness and size of the loop of the sigmoid colon depend on it.
The relationship of the rectum to the pelvic peritoneum at its various levels changes. The pelvic part is more or less covered with a serous membrane. The perineal part is devoid of peritoneal cover. The uppermost (supra-ampullary) part, starting at the level of the third sacral vertebra, is completely surrounded by serous tissue and has a short and narrow mesentery.
The left flexure of the colon is connected to the diaphragm by a horizontally located peritoneal phrenic-colic fold (sometimes referred to as the diaphragmatic-colic ligament, lig. phrenicocolicum).
For a more convenient study of the topography of the peritoneum and organs of the abdominal cavity, a number of topographic-anatomical definitions are used that are used in the clinic and do not have either Latin terms or their Russian equivalents.
Peritoneal folds, ligaments, mesenteries and organs create depressions, pouches, bags and sinuses that are relatively isolated from each other in the peritoneal cavity.
Based on this, the peritoneal cavity can be divided into an upper floor and a lower floor.
The upper floor is separated from the lower floor by the horizontally located mesentery of the transverse colon (at the level of the II lumbar vertebra). The mesentery is the lower boundary of the upper floor, the diaphragm is the upper, and the lateral walls of the abdominal cavity limit it on the sides.
The lower floor of the peritoneal cavity is bounded above by the transverse colon and its mesentery, on the sides by the side walls of the abdominal cavity, and below by the peritoneum covering the pelvic organs.
In the upper floor of the peritoneal cavity, there are subphrenic recesses, recessus subphrenici, subhepatic recesses, recessus subhepatici, and omental bursa, bursa omentalis.
The subdiaphragmatic recess is divided into right and left parts by the falciform ligament. The right part of the subphrenic recess is a gap in the peritoneal cavity between the diaphragmatic surface of the right lobe of the liver and the diaphragm. At the back it is bounded by the right part of the coronary ligament and the right triangular ligament of the liver, on the left by the falciform ligament of the liver. This depression communicates with the lower right subhepatic space, the right paracolic sulcus, then with the iliac fossa and through it with the small pelvis. The space under the left dome of the diaphragm between the left lobe of the liver (diaphragmatic surface) and the diaphragm is the left subphrenic recess.
On the right it is limited by the falciform ligament, on the back by the left part of the coronary and left triangular ligaments. This recess communicates with the lower left subhepatic recess.
The space under the visceral surface of the liver can be conditionally divided into two sections - right and left, the boundary between which can be considered the falciform and round ligaments of the liver. The right subhepatic recess is located between the visceral surface of the right lobe of the liver and the transverse colon and its mesentery. At the back, this depression is limited by the parietal peritoneum (hepatorenal ligament, lig. hepatorenale). Laterally, the right subhepatic recess communicates with the right paracolic sulcus, and in depth, through the omental foramen, with the omental bursa. The section of the subhepatic space, located deep at the posterior edge of the liver, to the right of the spinal column, is called the hepatorenal recess, recessus hepatorenalis.


The left subhepatic recess is a gap between the lesser omentum and the stomach on one side and the visceral surface of the left lobe of the liver on the other. Part of this space, located outward and somewhat posterior to the greater curvature of the stomach, reaches the lower edge of the spleen.
Thus, the right subphrenic and right subhepatic recesses surround the right lobe of the liver and the gallbladder (facing here outside surface duodenum). In topographic anatomy they are combined under the name “hepatic bursa”. In the left subdiaphragmatic and left subhepatic recess there are the left lobe of the liver, the lesser omentum, and the anterior surface of the stomach. In topographic anatomy, this section is called the pregastric bursa. The omental bursa, bursa omentalis, is located behind the stomach. To the right it extends to the omental foramen, to the left - to the hilum of the spleen. The anterior wall of the omental bursa is the lesser omentum, the posterior wall of the stomach, the gastrocolic ligament, and sometimes the upper part of the greater omentum, if the descending and ascending leaves of the greater omentum are not fused and there is a gap between them, which is considered as a downward continuation of the omental bursa.
The posterior wall of the omental bursa is the parietal peritoneum, covering the organs located on the posterior wall of the abdominal cavity: the inferior vena cava, abdominal aorta, left adrenal gland, upper end of the left kidney, splenic vessels and below - the body of the pancreas, which occupies the largest space of the posterior wall of the omental bursa.
The upper wall of the omental bursa is the caudate lobe of the liver, the lower wall is the transverse colon and its mesentery. The left wall is the gastrosplenic and diaphragmatic-splenic ligaments. The entrance to the bag is the omental opening, foramen epiploicum (omentale), located on the right side of the bag behind the hepatoduodenal ligament. This hole allows 1-2 fingers through. Its anterior wall is the hepatoduodenal ligament with the vessels located in it and the common bile duct. The posterior wall is the hepatorenal ligament, behind which are the inferior vena cava and the upper end of the right kidney. The lower wall is formed by the peritoneum, which passes from the kidney to the duodenum, and the upper wall is formed by the caudate lobe of the liver. The narrow section of the bursa closest to the opening is called the vestibule of the omental bursa, vestibulum bursae omentalis; it is bounded by the caudate lobe of the liver above and the upper part of the duodenum below.
Behind the caudate lobe of the liver, between it and the medial leg of the diaphragm, covered with parietal peritoneum, there is a pocket - the superior omental recess, recessus superior omentalis, which is open at the bottom towards the vestibule. Down from the vestibule, between the posterior wall of the stomach and the gastrocolic ligament in front and the pancreas covered with the parietal peritoneum and the mesentery of the transverse colon at the back is the lower omental recess, recessus inferior omentalis. To the left of the vestibule, the cavity of the omental bursa is narrowed by the gastropancreatic fold of the peritoneum, plica gastropancreatica, running from the upper edge of the omental tubercle of the pancreas upward and to the left, to the lesser curvature of the stomach (it contains the left gastric artery, a. gastrica sinistra). The continuation of the lower recess to the left is the sinus, located between the gastrosplenic ligament (in front) and the phrenic-splenic ligament (back), which is called the splenic recess, recessus lienalis.
In the lower floor of the peritoneal cavity, on its posterior wall, there are two large mesenteric sinuses and two paracolic grooves. Here, the lower layer of the mesentery of the transverse colon, down from the root, passes into the parietal layer of the peritoneum, lining the posterior wall of the mesenteric sinuses.
The peritoneum, covering the posterior wall of the abdomen in the lower floor, passing on to the small intestine, surrounds it on all sides (except for the duodenum) and forms the mesentery of the small intestine, mesenterium. The mesentery of the small intestine is a double layer of peritoneum. The root of the mesentery, radix mesenterii, goes obliquely from top to bottom from the level of the II lumbar vertebra on the left to the sacroiliac joint on the right (the place where the ileum enters the cecum). The length of the root is 16-18 cm, the width of the mesentery is 15-17 cm, however, the latter increases in the parts of the small intestine most distant from the posterior wall of the abdomen. Along its course, the root of the mesentery crosses at the top the ascending part of the duodenum, then the abdominal aorta at the level of the IV lumbar vertebra, the inferior vena cava and the right ureter. Along the root of the mesentery there are, following from top left to bottom and to the right, the superior mesenteric vessels; The mesenteric vessels give off intestinal branches between the layers of the mesentery to the intestinal wall. In addition, between the layers of the mesentery there are lymphatic vessels, nerves, and regional lymph nodes. All this largely determines that the duplication plate of the mesentery of the small intestine becomes dense and thickened.
The mesentery of the small intestine divides the peritoneal cavity of the lower floor into two sections: the right and left mesenteric sinuses.

The right mesenteric sinus is bounded above by the mesentery of the transverse colon, on the right by the ascending colon, and on the left and below by the mesentery of the small intestine. Thus, the right mesenteric sinus has the shape of a triangle and is closed on all sides. Through the parietal peritoneum lining it, the lower end of the right kidney (to the right) is contoured and visible at the top under the mesentery of the colon; adjacent to it is the lower part of the duodenum and the lower part of the head of the pancreas, surrounded by it. Below in the right sinus the descending right ureter and the ileocolic artery and vein are visible.
Below, at the point where the ileum enters the cecum, an ileocecal fold, plica ileocecalis, is formed. It is located between the medial wall of the cecum, the anterior wall of the ileum and the parietal peritoneum, and also connects the medial wall of the cecum with the lower wall of the ileum above and with the base of the appendix below. In front of the ileocecal angle there is a fold of the peritoneum - the vascular cecal fold, plica cecalis vascularis, in the thickness of which the anterior cecal artery passes. The fold extends from the anterior surface of the mesentery of the small intestine and approaches the anterior surface of the cecum. Between the upper edge of the appendix, the ileum and the wall of the medial portion of the bottom of the cecum there is the mesentery of the appendix, mesoappendix. Feeding vessels pass through the mesentery, a. et v. appendiculares, and regional lymph nodes and nerves are embedded. Between the lateral edge of the bottom of the cecum and the parietal peritoneum of the iliac fossa there are cecal folds, plicae cecales.
Under the ileocecal fold lie the pockets located above and below the ileum: the upper and lower ileocecal recesses, recessus ileocecalis superior, recessus ileocecalis inferior. Sometimes under the bottom of the cecum there is a retrocecal recess, recessus retrocecalis.
To the right of the ascending colon is the right paracolic groove. It is limited externally by the parietal peritoneum of the lateral wall of the abdomen, on the left by the ascending colon; communicates downward with the iliac fossa and the peritoneal cavity of the small pelvis. At the top, the groove communicates with the right subhepatic and subphrenic recesses. Along the groove, the parietal peritoneum forms transverse folds connecting the upper right bend of the colon with the lateral wall of the abdomen and the right diaphragmatic-colic ligament, usually weakly expressed, sometimes absent.
The left mesenteric sinus is bounded above by the mesentery of the transverse colon, on the left by the descending colon, and on the right by the mesentery of the small intestine. Inferiorly, the left mesenteric sinus communicates with the peritoneal cavity of the small pelvis. The sinus has an irregular quadrangular shape and is open downward. Through the parietal peritoneum of the left mesenteric sinus, the lower half of the left kidney is visible and contoured at the top, below and medially in front of the spine - the abdominal aorta and to the right - the inferior vena cava and the initial segments of the common iliac vessels. To the left of the spine, the left artery of the testicle (ovary), the left ureter and the branches of the inferior mesenteric artery and vein are visible. In the upper medial corner, around the beginning of the jejunum, the parietal peritoneum forms a fold that borders the intestine from above and to the left - this is the superior duodenal fold (duodeno-jejunal fold), plica duodenalis superior (plica duodenojejunalis). To the left of it is the paraduodenal fold, plica paraduodenalis, which is a semilunar fold of the peritoneum located at the level of the ascending part of the duodenum and covering the left colon artery. This fold limits the front of the unstable paraduodenal recess, recessus paraduodenalis, the posterior wall of which is made up of the parietal peritoneum, and to the left and below runs the lower duodenal fold (duodenal-mesenteric fold), plica duodenalis inferior (plica duodenomesocolica), which is a triangular fold of the parietal peritoneum, passing on the ascending part of the duodenum.
To the left of the root of the mesentery of the small intestine, behind the ascending part of the duodenum, there is a peritoneal fossa - a retroduodenal recess, recessus retroduodenalis, the depth of which can vary. To the left of the descending colon is the left paracolic groove; it is limited on the left (laterally) by the parietal peritoneum lining the lateral wall of the abdomen. Downwards, the groove passes into the iliac fossa and then into the pelvic cavity. Upwards, at the level of the left flexure of the colon, the groove is crossed by a constant and well-defined phrenic-colic fold of the peritoneum.
Below, between the bends of the mesentery of the sigmoid colon, there is a peritoneal intersigmoid recess, recessus intersigmoideus.
You might be interested in this read:
Perhaps the world would seem more attractive to us if we were able to see what remains hidden from us. Man is the most interesting and complex organism on the planet. It is capable of performing several functions simultaneously. Each organ within us has its own responsibilities and works harmoniously with each other. For example: pumps blood, the brain develops a process that allows you to think. In order to understand our body well, we need to know what the location of the abdominal organs is.
In contact with
The structure of the internal organs of the abdomen
The anatomy of the abdomen is conventionally divided into 2 parts: external and internal.
To the outside applies:
- head,
- breast,
- torso,
- upper and lower limbs.
To the second:
- brain,
- lungs,
- components of the gastrointestinal tract,
Structure of the abdominal cavity pretty hard e - these are the organs of the abdominal cavity, which are located below the diaphragm and make up the following parts:
- anterior wall of the peritoneum,
- muscle parts,
- broad abdominal muscles,
- lumbar part.
To the number abdominal organs people include:
- stomach,
- spleen,
- gallbladder,
- human intestines.
Attention! When a person is born, after the umbilical cord is removed, a scar remains in the center of the abdomen. It's called the navel.
So, let's consider in detail what is the location of the human internal organs in the abdominal cavity, what is their appearance and functionality.
Earlier we recalled that the stomach, pancreas, gallbladder, kidneys, adrenal glands, spleen and intestinal tract are all constituent organs abdominal cavity. What is each of them?
The stomach is the so-called muscle, which is located on the left under the diaphragm (a diagram of the stomach is shown in the pictures below). This component of the human gastrointestinal tract tends to stretch, in its normal state size is 15 cm. When it is filled with food, it can put pressure on the pancreas.
One of the main functions is the digestion of food, for which gastric juice is used. Most people have stomach problems; one of the main diseases is gastritis, in which the following symptoms are observed:
- bad breath,
- heartburn,
- bloating in the abdominal area,
- frequent belching.
Important! The inner lining of the stomach wall is renewed every 3-4 days. The mucous coating of the stomach wall quickly dissolves under the influence of gastric juice, which is a strong acid.
Pancreas located below the stomach, participates in the production of enzymes, ensures protein, fat and carbohydrate metabolism. The gland also releases insulin into the blood. If the production of this hormone is disrupted, a person develops a disease - diabetes. The main symptoms of this pathology may be:
- constant feeling of thirst,
- frequent urination,
- sweat takes on a sweet taste.
If the pancreas malfunctions, the entire human gastrointestinal tract suffers. The size of the gland is average about 22 cm. Its head is the largest part, measuring 5 cm and thickness up to 3 cm.
Symptoms of disruption of the proper functioning of the human pancreas and gastrointestinal tract may include:
- rumbling in the stomach,
- feeling of nausea,
- flatulence (release of gases),
- pain in the abdominal area near the hypochondrium,
- decreased appetite.
Throughout the day, the pancreas produces 2 liters of pancreatic juice(this is 10 times more than is required for normal digestion of food).
 The gallbladder is a small pear-shaped organ that is located in a person in the right hypochondrium (lower edge of the costal arch on the right). It is located below the liver.
The gallbladder is a small pear-shaped organ that is located in a person in the right hypochondrium (lower edge of the costal arch on the right). It is located below the liver.
It is in the gallbladder that bile accumulates, which external signs resembles a viscous green liquid. By the bubble thin wall.
Despite the fact that the size of the bladder is very small, it plays a very important role in the body. When its functioning is disrupted, a person experiences a feeling of nausea, vomiting and pain on the right side. These symptoms may also indicate the progression of a disease such as an ulcer.
Also located in the peritoneum area are the kidneys, a paired organ. In humans, they are located in the lower posterior part of the peritoneum. The left kidney is slightly larger in size and is located above the right, which is considered normal.
So what does the organ look like? The buds look like beans. On average, they have parameters of 12 cm, weight approximately 160 g. For the body, they play a very significant role - help the recusal urine. A healthy person can pass one to two liters of urine per day.
When a person notices changes in the color of urine, this may be a signal that there is a problem with this organ. Pain in the lower back also appears, body temperature rises, and swelling appears. There are so-called “bags under the eyes”.
If the above symptoms are detected, you should immediately contact a specialist to avoid salt accumulation and the formation of kidney stones, as well as other complications in the form inflammatory processes. Kidneys require a lot of attention!
In humans, the adrenal glands, like the kidneys, are located on both sides of the posterior wall of the abdominal cavity. How the organs are located, the name speaks for itself - above the kidneys. Their functionality is to produce most hormones, including adrenaline. They regulate metabolism and help the body feel comfortable in stressful situations.
 Disruption of the adrenal glands can result from excessive or insufficient secretion of hormones. At the same time, it increases arterial pressure, potassium levels decrease, which can result in acute renal failure. If you have such symptoms, you should visit an endocrinologist.
Disruption of the adrenal glands can result from excessive or insufficient secretion of hormones. At the same time, it increases arterial pressure, potassium levels decrease, which can result in acute renal failure. If you have such symptoms, you should visit an endocrinologist.
The spleen is shaped like a bean. Its location is behind the stomach in the left upper lobe. Its parameters: length - 16 cm, width - 6 cm, weight - approximately 200 g.
The main function is to protect against infections, control metabolism, and filter damaged platelets and red blood cells. Due to the anatomical structure of the human abdomen, a diseased spleen does not always make itself felt. It often happens that when running a person experiences pain on the left side, under the rib. This means that blood has entered the general bloodstream. This problem is not terrible.
Important! If the pain moves to the chest area, this indicates that an abscess is developing. At the same time, the organ enlarges, which only a doctor can determine.
An aching and pulling pain that radiates to the lumbar region makes it clear that the person may have had a heart attack.
The arrangement of organs in the peritoneum is such that when the spleen reaches very large sizes, This palpable on the right in the area of the womb upon palpation. Such signs may accompany tuberculosis. The pain becomes impossible to bear. Dull pain can warn of the appearance of a tumor.
Gastrointestinal tract
Probably everyone asked themselves the question: “What does the gastrointestinal tract consist of?” In order for us to feel good, we need energy. This is why the gastrointestinal tract exists, which includes many organs. Incorrect operation of one of them can harm your health.
The gastrointestinal tract includes:
- throat,
- esophagus,
- stomach,
- intestines.
Initially, food is sent to the mouth, where it is chewed and mixed with saliva. Chewed food acquires a porridge-like consistency and is swallowed using the tongue. The food then goes down the throat.
Pharynx externally looks like a funnel, has a mouth-nose connection. From it, food components are sent to the esophagus.
The esophagus is the muscular tube. Its location is between the pharynx and stomach. The esophagus is covered with a shell of mucus, which contains many glands that saturate with moisture and soften food, due to which it easily penetrates into the stomach.
Processed food moves from the stomach to the intestines. We will tell you further where the human intestine is located and what functions are assigned to it.
Intestines
The intestine is a special organ that forms 2/3 immune system, processes the food received into energy and simultaneously produces more than twenty of its own hormones. Located in the abdominal cavity, general length is 4 meters. Its shape and structure changes depending on age. Anatomically, this organ is divided into the small and large intestines.
The diameter of the small intestine is 6 cm, gradually decreasing to 3 cm. On average, the size of the large intestine reaches 8 cm.
Anatomically, the small intestine is divided into three departments:
- duodenum,
- skinny,
- ileum.
 The duodenum originates from the stomach and ends in the jejunum. Bile comes from the gallbladder, and juice from the pancreas. It produces a large number of glands that help process food and protect it from damage and irritation. acidic substance.
The duodenum originates from the stomach and ends in the jejunum. Bile comes from the gallbladder, and juice from the pancreas. It produces a large number of glands that help process food and protect it from damage and irritation. acidic substance.
Lean - makes up about 2/5 of the entire length of the intestine. Its size is about 1.5 meters. For the fair sex it is shorter than for the stronger half. When a person dies, it stretches and is about 2.5 meters.
Ileum - located in the lower part of the small intestine, she's much thicker and has a more developed vascular system.
Painful symptoms of the small intestine include:
- weight loss;
- feeling of heaviness in the stomach;
- flatulence;
- upset (loose stools);
- soreness in the navel area.
As for the large intestine, it includes: the cecum, colon, sigmoid and rectum. This part of the body has a grayish tint, length - 2 meters, width -7 cm. Its main functions are: fluid absorption, regular excretion of feces.
The cecum is the widest part of the intestine, called the appendix. It contains organisms that help the functioning of the intestines. The bag-shaped area reaches 8 cm in length.
The colon is divided into: descending, transverse and ascending. Its diameter is 5 cm, length is 1.5 meters.
Sigmoid - originates at the beginning of the small pelvis and directed transversely- to the right. In a fully formed person, it reaches about 55 cm.
The direct line is the final link in the process of processing food by the body. It has this name because it does not bend. Its functionality is the accumulation and removal of food waste. The rectum reaches 15 cm in length.
Accumulate in the rectum defecation products which are expelled through the anus.
If you experience painful sensations during bowel movements, there are blood impurities in the stool, frequent diarrhea is replaced by constipation, or weight loss is observed - this is a reason to consult a specialist.
Where is which organ located in a person?
Anatomy of the abdominal organs
15.02.2020
A new section has been opened on the website in the “Esoteric Heritage” Menu:
At the moment, in this section we post current materials from our forum, calling them “Chapters” in no particular order, which can later be combined into new book dedicated to the topic of the section.
06.04.2019
Individual work with the Philosopher, 2019
We offer for all readers of our website and forum who are looking for answers to questions about the world, about the Purpose and Meaning of human life, a new format of work... - “Master Class with the Philosopher”. For questions, please contact the Center by email:
15.11.2018
Updated manuals on Esoteric Philosophy.
We have summed up the results research work Project for 10 years (including work on the forum), posting them in the form of files in the section of the website “Esoteric Heritage” - “Philosophy of Esoterics, our manuals since 2018”.
The files will be edited, adjusted and updated.
The forum has been cleared of historical posts and is now used exclusively for interaction with Adepts. No registration is required to read our website and forum.
For any questions you may have, including those related to our research, you can write to the email of the Center Masters This address Email protected from spam bots. You must have JavaScript enabled to view it.
02.07.2018
Since June 2018, within the framework of the Esoteric Healing group, the lesson “Individual Healing and working with Practitioners” has been taking place.
Anyone can take part in this direction of the Center’s work.
Details at .
30.09.2017
Seeking help from the Practical Esoteric Healing group.
Since 2011, a Group of Healers has been working at the Center in the direction of “Esoteric Healing” under the leadership of the Reiki Master and the Oracle Project.
In order to ask for help, write to our email with the subject “Contacting the Reiki Healers Group”:
- This email address is being protected from spambots. You must have JavaScript enabled to view it.
- "The Jewish Question"
- "The Jewish Question"
- "The Jewish Question"
- "The Jewish Question"
- "The Jewish Question"
- "The Jewish Question"
27.09.2019
Updates in the site section - "Esoteric Heritage" - "Hebrew - learning an ancient language: articles, dictionaries, textbooks":
- "The Jewish Question"
Popular materials
- Atlas of the human physical body
- Ancient copies of the Old Testament (Torah)
- “Yahweh against Baal - chronicle of a coup” (A. Sklyarov, 2016)
- Types of Monads - The Human Genome, theories about the emergence of various races and our conclusions about the creation of various types of Monads
- Fierce fight for Souls
- George Orwell "Thoughts on the Road"
- Table of psychological equivalents of Louise Hay's diseases (all parts)
- Has time begun to shrink and run faster? Inexplicable facts of decreasing hours in the day.
- About hypocrisy and lies... - illusions and reality, using the example of research on social networks...
- Simpletons abroad, or the path of new pilgrims. Excerpts from Mark Twain's book on Palestine (1867)
- The unity and monotony of monumental structures scattered throughout the world. Contradictions with the official version of the construction of St. Petersburg and its environs. Megalithic and polygonal masonry in some structures. (selection of articles)
- How a Komsomolskaya Pravda journalist said goodbye to glasses forever in seven weeks. (parts 1-7)
- Page not found
- Chimeras of new times - about genetically modified products
- Esoteric Approach to Religion (Philosopher)
- Apocryphal Gospel of Thomas about the childhood of Yeshua (Jesus Christ)
- Islamization of countries and the transition from Christianity to Islam, a selection of press materials
- The world is tired of Jews
- Vasily Grossman. The story "Everything Flows"
- Secret program for studying Mars. Media: NASA is hiding the whole truth about Mars from earthlings. There is evidence (selection of materials)
- Human intelligence began to slowly decline
- Materials for the study of parallels between Sumerian texts and the Torah. According to Sitchin's books
Atlas-drawings of the structure: spine, internal organs of the gastrointestinal tract, genitourinary system, head, nervous and immune systems
1. Spine (spinal column, sacrum, coccyx)
The spinal column (columna vertebralis) is the real basis of the skeleton, the support of the whole organism.
How many vertebrae?
In total, the spinal column has 32-34 vertebrae, separated by intervertebral discs and slightly different in their structure.
In accordance with the location and structural features of the spinal column, five types of vertebrae are distinguished: 7 cervical, 12 thoracic, 5 lumbar, 5 sacral and 3-5 coccygeal
1.1. Spinal column right view

1 - cervical lordosis;
2 - thoracic kyphosis;
3 - lumbar lordosis;
4 - sacral kyphosis;
5 - protruding vertebra;
6 - spinal canal;
7 - spinous processes;
8 - vertebral body;
9 - intervertebral foramina;
10 - sacral canal
1.2. Spinal column front view

1 - cervical vertebrae;
2 - thoracic vertebrae;
3 - lumbar vertebrae;
4 - sacral vertebrae;
5 - atlas;
6 - transverse processes;
7 - coccyx I cervical vertebra Atlas I cervical vertebra, or atlas (Fig. 5), the body is absent; its lateral masses (massae laterales) are connected by two arches - anterior (arcus anterior) and posterior (arcus posterior).
The upper and lower planes of the lateral masses have articular surfaces (upper and lower), through which the first cervical vertebra is connected to the skull and the second cervical vertebra, respectively.
Sacrum bone

A - front view; B - rear view:
1 - base of the sacrum;
2 - upper articular processes of the 1st sacral vertebra;
3 - anterior sacral foramina;
4 - transverse lines;
5 - apex of the sacrum;
6 - sacral canal;
7 - posterior sacral foramina;
8 - median sacral ridge;
9 - right ear-shaped surface;
10 - intermediate sacral ridge;
11 - lateral sacral ridge;
12 - sacral fissure;
13 - sacral horns
 The lateral parts of the sacrum are formed by fused transverse processes and rudiments of the ribs of the sacral vertebrae.
The lateral parts of the sacrum are formed by fused transverse processes and rudiments of the ribs of the sacral vertebrae.
The upper sections of the lateral surface of the lateral parts have articular ear-shaped surfaces (facies auricularis), through which the sacrum articulates with the pelvic bones. The anterior pelvic surface of the sacrum is concave, with noticeable traces of fusion of the vertebrae (look like transverse lines), forms the posterior wall of the pelvic cavity. Four lines , marking the fusion of the sacral vertebrae, end on both sides with the anterior sacral foramina.
The posterior (dorsal) surface of the sacrum, which also has 4 pairs of posterior sacral foramina, is uneven and convex, with a vertical ridge running through the center.
This median sacral ridge is a trace of the fusion of the spinous processes of the sacral vertebrae. To the left and right of it are the intermediate sacral ridges, formed by the fusion of the articular processes of the sacral vertebrae. The fused transverse processes of the sacral vertebrae form a paired lateral sacral ridge. The paired intermediate sacral ridge ends at the top with the usual superior articular processes of the first sacral vertebra, and at the bottom with the modified lower articular processes of the fifth sacral vertebra.
These processes, the so-called sacral horns, serve to articulate the sacrum with the coccyx. The sacral horns limit the sacral fissure - the exit of the sacral canal.
Coccyx

A - front view; B - rear view:
1 - coccygeal horns;
2 - outgrowths of the body of the first coccygeal vertebra;
3 - coccygeal vertebraeThe coccyx (os coccygis) consists of 3-5 underdeveloped vertebrae (vertebrae coccygeae), having (with the exception of I) the shape of oval bone bodies that finally ossify at a relatively late age.
The body of the first coccygeal vertebra has outgrowths directed to the sides, which are rudiments of transverse processes; At the top of this vertebra there are modified upper articular processes - the coccygeal horns (cornua coccygea), which connect to the sacral horns. By origin, the coccyx is a rudiment of the caudal skeleton.
2. Structure of internal organs

2.1. The heart (cor) is the main element of the cardiovascular system, ensuring blood flow in the vessels.
A distinctive feature is the ability to operate automatically.
Heart position

1 - left subclavian artery;
2 - right subclavian artery;
3 - thyrocervical trunk;
4 - left common carotid artery;
5 - brachiocephalic trunk;
6 - aortic arch;
7 - superior vena cava;
8 - pulmonary trunk;
9 - pericardial sac;
10 - left ear;
11 - right ear;
12 - arterial cone;
13 - right lung;
14 - left lung;
15 - right ventricle;
16 - left ventricle;
17 - apex of the heart;
18 - pleura;
19 - diaphragm
2.2. Diagram of the course of the peritoneum - Organs of the gastrointestinal tract (gastrointestinal tract)
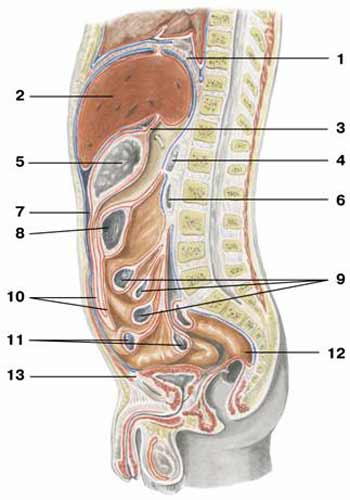
1 - diaphragm;
2 - liver;
3 - small seal;
4 - pancreas;
5 - stomach;
6 - duodenum;
7 - peritoneal cavity;
8 - transverse colon;
9 - jejunum;
10 - large oil seal;
11 - ileum;
12 - rectum;
13 - retrovisceral space
2.3 Abdominal organs 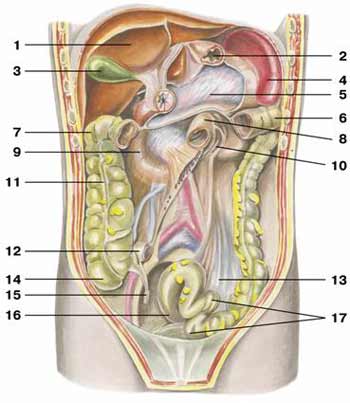
1 - liver;
2 - stomach;
3 - gallbladder;
4 - spleen;
5 - pancreas;
6 - left flexure of the colon;
7 - right flexure of the colon;
8 - superior flexure of the duodenum;
9 - relief of the duodenum;
10 - ascending part of the duodenum;
11 - ascending colon;
12 - ileum;
13 - mesentery of the sigmoid colon;
14 - cecum;
15 - appendix;
16 - rectum;
17 - sigmoid colon
2.4 Urinary and genital organs
The urinary organs, which are also called excretory organs, cleanse the body of toxins (salts, urea, etc.) formed as a result of metabolism.
Urinary organs front view

1 - diaphragm;
2 - left adrenal gland;
3 - right adrenal gland;
4 - left kidney;
5 - right kidney;
6 - left ureter;
7 - right ureter;
8 - rectum;
9 - bladder
2.5. Diagram of the male genitourinary apparatus

1 - left kidney;
2 - cortex;
3 - right kidney;
4 - renal pyramids;
5 - kidney gate;
6 - renal pelvis;
7 - left ureter;
8 - apex of the bladder;
9 - bottom of the bladder;
10 - body of the bladder;
11 - seminal vesicle;
12 - prostate gland;
13 - body of the penis;
14 - root of the penis;
15 - vas deferens;
16 - appendage;
17 - head of the penis;
18 - testicle;
19 - testicular lobules
Male genital organs side view

Man still remains an extremely complex structured organism on the planet. Our body - unique system, in which all its parts work harmoniously and perform a number of functions simultaneously. Each organ in our body has its own task and performs it: the lungs enrich blood cells with oxygen, the heart drives oxygenated blood throughout the body to deliver it to each cell, the brain controls all cognitive processes.
The structure of both internal organs and the entire body is studied by human anatomy, which is divided into internal and external.

The external structure of a person combines those parts of the body that we can see with our own eyes without any devices. The external anatomical structure includes organs such as the head, neck, torso, chest, back, upper and lower limbs. Internal anatomy describes the location of the human internal organs in the body; they cannot be seen with the naked eye.
The structure of our body is in many ways the same as that of mammals. This fact is not difficult to explain, since according to evolutionary theory, humans can be one of the branches of mammalian development. Man developed simultaneously with animals in similar natural conditions, which ensured similarities in the structure of cells, tissues, internal organs and their systems.
Structure of internal organs: brain

The brain is the most complex internal organ, the complex structure of which puts us several steps higher in development than all other creatures on the planet. The brain and the complex of neurons is the central nervous system, under the control of which all body functions are located and the thought process is ensured. The brain is positioned as a collection of nerve fibers that form a complex stable system. It includes the two cerebral hemispheres, the cerebellum and the pons.
Even now, experts say that human brain not even half studied. During the formation of anatomy as a science, the greatest difficulties arose precisely with the description of the processes occurring in the nervous tissue that forms the brain.
Main parts of the brain:
- Large hemispheres occupy the largest part of the brain volume. Through them, control occurs at all stages of thought processes. It is thanks to the action of the cerebral hemispheres that we make conscious movements;
- Two pons. One of the bridges is located under the cerebellum, almost at the base of the skull, and performs the task of receiving and transmitting nerve impulses. The second bridge is located even lower, has an oblong shape and ensures the transmission of signals from the spinal cord;
- Cerebellum. A significant part of the brain that determines the ability to keep the body in balance. Controls muscle reflexes. For example, when touching something hot, we withdraw our hand even before we have time to realize what has happened. It is these reflexes that are controlled by the cerebellum.
Human abdominal organs

The abdominal cavity is defined as the space that is delimited from the top by the diaphragm from the chest cavity; it is closed from the front and sides by the abdominal muscles, and from the back it is protected by the column of the spine and the muscle tissue located there. The abdominal cavity is also called the abdominal cavity.
From below, the abdominal cavity smoothly passes to the pelvic cavity. There is a complex of internal organs that perform various important functions, as well as nerve endings and large blood vessels. Diseases of the abdominal organs are the most common cases in practical medicine and have big influence on the entire human body, therefore, the speed of making a correct diagnosis and the patient’s life depend on knowledge about them.
Some of the organs located inside the abdominal cavity are completely or partially covered with a special membrane, but some of them do not have it at all.
This shell has significant elasticity and is characterized by a specific absorption ability. Serous fluid is produced here, which, acting as a lubricant, reduces the amount of friction between the organs.

Organs of the abdominal cavity
- Stomach- a muscular organ shaped like a bag. This is one of the main organs of the food digestion system, essentially being a continuation of the esophagus in the abdominal cavity. The walls of the stomach produce a special complex of biologically active substances and enzymes, called gastric juice, which actively breaks down nutrients. The acidity of gastric juice can indicate the condition of the entire gastrointestinal tract as a whole.
- Intestines. This is the longest part digestive system. It begins with the outlet of the stomach and ends with the excretory system. Inside the abdominal cavity, the intestines are located in the form of peculiar loops. The main task of this organ remains to digest food and remove unnecessary substances from the body. The intestine is divided into large, small and rectum.
- Kidneys- just like the lungs, a paired organ that is localized in the lumbar region and, if you look at the photo, resembles beans in shape. They ensure the maintenance of homeostatic balance in the body and are also part of the urinary system.
- Adrenal glands. The satellite organs of the kidneys, also paired, are located on the right and left in the abdominal cavity. Their main task is to regulate the functionality of the endocrine and hormonal systems. The adrenal glands produce a large number of hormones - more than 25, which include adrenaline, corticosteroids and other substances. The adrenal glands also transmit impulses from the nervous system, which are captured by the medulla that fills these organs. Here, the processes of inhibition and excitation characteristic of stressful conditions are regulated.
- Liver known as the largest gland in our body. It is located directly below the diaphragm and is divided into two lobes. The liver neutralizes toxic and harmful substances to the body, so it is the first organ that suffers if a person has bad habits. The liver also takes part in blood circulation and influences digestive processes. In the process of functioning, there is a close connection between the liver and the gallbladder.
- Bladder is also located in the abdominal cavity and is a kind of bag in which urine accumulates, which is subsequently removed from the body through the efforts of the excretory system. The bladder is located in the groin area behind the pubic bone. The bladder also has a significant impact on digestion. Disturbances in its functioning can lead to such unpleasant consequences as discomfort, nausea and vomiting. This also often leads to the development of peptic ulcers of the stomach and intestines.
- Pancreas. It has the ability to produce special substances and enzymes that improve the speed and quality of food digestion. This organ is located on the left behind the stomach, in the upper half of the abdominal cavity. One of its main tasks is to provide the body with a natural hormone – insulin. When pancreatic function is impaired, diabetes mellitus develops.

An important hematopoietic organ of the abdominal cavity is the spleen; if you look at a model of a person with organs, it can be found above the diaphragm. This is a unique organ that has the ability to change its size depending on the volume of blood flow. The spleen also performs a protective function in the body.
Significant differences in the structure of the male and female abdominal cavity
The arrangement of the abdominal organs has a constant structure, characteristic of any person of any nationality. Some structural features are distinguished in childhood and adulthood, but most of the differences are determined by gender.
In men, the abdominal cavity is defined as a closed system, but in women it is not a closed space, since in female body communication occurs with the uterine region using the fallopian tubes. In addition, in the female body, the abdominal cavity is able to communicate with the external environment through the vaginal cavity.
Organs of the chest cavity

The chest is the most important protective structure in our body, which protects the most significant organ in the human body - the heart and the largest blood vessels that connect to it. Most of the chest cavity is occupied by the lungs, which saturate the blood with oxygen and remove carbon dioxide, which is harmful to the body. Also located here is the diaphragm, which is a flat broad muscle, one of the functions of which is to differentiate the chest and abdominal cavity. Let's take a closer look at the location of human organs located in the chest cavity.
The heart is a hollow muscular organ located in the chest between the lungs and shifted to the left side. It is easy to imagine the size of the heart if you clench the hand of an adult into a fist. On the one hand, the heart performs one simple function - it pumps blood into the arteries and receives venous blood, on the other hand, without this function our body could not exist.
Basic facts about the structure and function of the heart

- The heart produces the movements necessary to pump blood into the vessels through the work of the left and right ventricles;
- The arrangement of the heart inside the chest is very curious and is called oblique presentation. This means that the narrower part of this organ looks down and to the left, and the wider part looks up and to the right;
- The right ventricle of the heart is slightly smaller than the left;
- The main vessels arise from the wide part of the heart (or its base). The heart is never at rest, since it needs to constantly pump blood into the vessels, which carries oxygen and nutrients to all cells of the body;
- On the outside, this muscular organ is covered with pericardium, a special type of tissue in the outer part of which blood vessels are located. The inner layer of the pericardium fits tightly to the heart.
Lung structure

The lungs are the largest paired organ, not only located in the chest cavity, but also in the human body as a whole. Both lungs - left and right, are identical in appearance, but nevertheless, their anatomy and functions have significant differences.
The left lung can be divided into only two lobes, while the right lung can be divided into as many as three. Also, the lung, located in the chest on the left, is distinguished by the presence of a bend. The main task of the lungs remains the processing and oxygenation of blood cells, as well as the removal of carbon dioxide formed during the breathing process, the presence of which is dangerous for the entire body.
Also in the chest cavity is the trachea, which acts as an air duct through which oxygen enters the lungs. It is located from top to bottom and connects the larynx with the bronchi. This organ is a complex of cartilaginous half-rings and connective ligaments; a mucus-covered trachea is located on the posterior wall of the trachea. muscle. The trachea in the lower section is divided into bronchi, which are essentially its continuation. Air enters the lungs through the bronchi. In the internal composition of the lung there are many bronchi, whose branches represent complex structure. The trachea also performs protective and cleansing functions.
The thoracic cavity also contains the esophagus, a muscular organ that connects the larynx to the stomach and ensures the supply of food.
Caring for the body is the key to health

Despite the extensive knowledge of humanity and its own anatomy, the human body still remains the most important object of study and experimentation. We have not yet solved all of its mysteries; there are a great many of them ahead.
At the same time, the instinct of self-preservation, protection of the entire body and internal organs is inherent in all living beings from the very beginning. However, people often forget to treat their body with due respect. Not only leading an unhealthy lifestyle and having bad habits, but also doing heavy physical labor or other situations that require the body to work at the limit of its capabilities can cause disruptions in the functioning of internal organs and lead to diseases. Therefore, do not forget about caring for your body.